Rib Fracture
Rib fractures are painful injuries caused by direct trauma, falls, or accidents. While most heal independently in 6-8 weeks, proper management is essential to prevent complications like flail chest or pneumothorax. Early diagnosis and pain control optimize healing.
Get Urgent Evaluation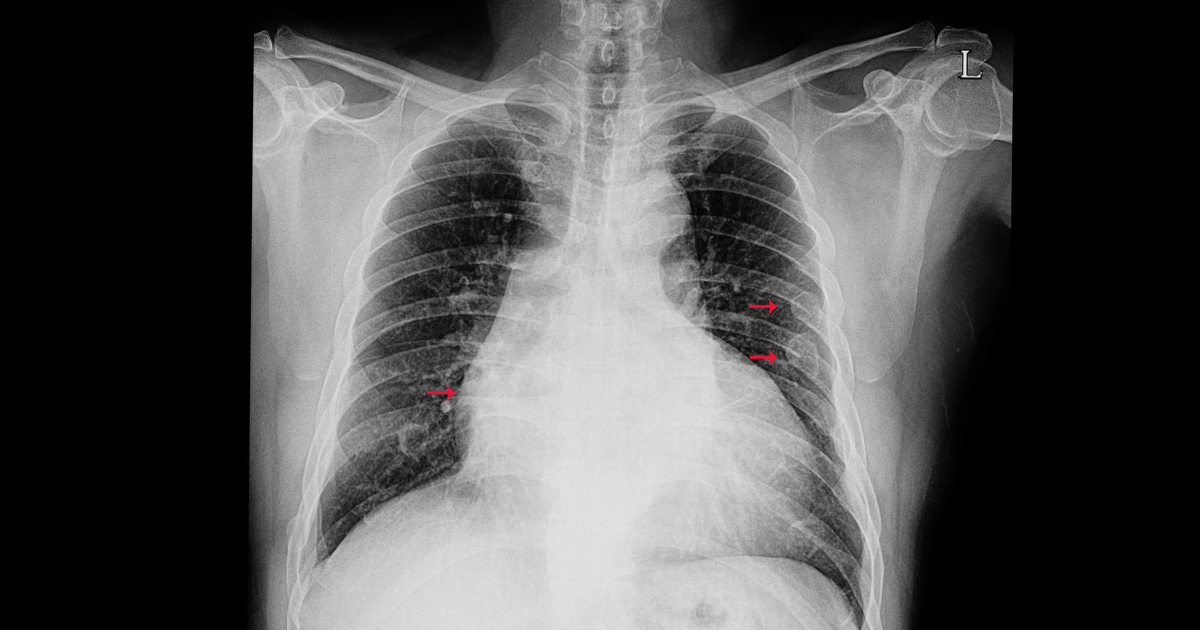
What Is a Rib Fracture?
A rib fracture is a break in one of the 12 pairs of bones forming the rib cage. Ribs protect the heart, lungs, and other vital organs. Rib fractures typically result from direct blunt trauma to the chest, such as from motor vehicle accidents, falls, or sports injuries.
Most rib fractures are uncomplicated and heal naturally within 6-8 weeks with appropriate pain management and rest. However, multiple rib fractures (flail chest) or fractures with complications can be serious and require more intensive management.
The main concern with rib fractures is not the bones themselves, but potential injuries to underlying structures. Complications can include pneumothorax (collapsed lung), hemothorax (bleeding into chest cavity), and injury to organs like the spleen, liver, or lungs.
At MyDoc Urgent Care, we provide rapid evaluation, imaging, and comprehensive management of rib fractures with emphasis on pain control and preventing serious complications.
Typical Symptoms
Sharp, severe chest wall pain
Pain worse with deep breathing
Pain worse with coughing or sneezing
Pain worse with movement or exertion
Painful respiration (dyspnea)
Tenderness over fracture site
Swelling or bruising over ribs
Shallow breathing (splinting)
Pain radiating to shoulder blade
Difficulty lying flat
Pain with twisting or bending
Audible cracking sensation (crepitus)
Frequently Asked Questions
What is urgent care and how does it work?
Urgent care centers are designed to treat those who need attention quickly but don't require an emergency room visit. At MyDoc Urgent Care, you can walk in without an appointment and receive prompt medical attention for a wide range of non-life-threatening conditions. Our clinics are open 7 days a week, 12 hours a day (8:00 AM – 8:00 PM), providing extended access beyond typical primary care hours. We offer services such as treatment for minor injuries and illnesses, diagnostic testing, vaccinations, and preventive care. Our goal is to bridge the gap between your primary care doctor and the emergency room, ensuring you get the care you need, when you need it.
Who do we treat?
We treat patients of all ages, from infants and children to adults and seniors. Whether you have a minor illness, need a physical exam, or require urgent attention for an injury, our team is equipped to help. We welcome both long-time residents and visitors to the area. Our providers are experienced in pediatric, adult, and geriatric care, and we strive to create a welcoming, compassionate environment for every patient. If you have a chronic condition and need prompt care, we can help manage your symptoms and coordinate with your primary care provider if needed.
How do I get started?
Getting care at MyDoc Urgent Care is easy. Simply walk in to any of our locations during business hours—no appointment is necessary. If you have questions or want to check wait times, you can call us at (718) 401-1510. For added convenience, you can also check in online to reduce your wait time. When you arrive, our friendly staff will help you register and guide you through the process. Most visits are completed in under an hour, so you can get back to your day quickly.
How does Urgent Care compare to the ER or a Primary Care Doctor?
Urgent care is designed for non-life-threatening conditions that require prompt attention but are not severe enough for the emergency room. The average wait time for a primary care appointment can be over 20 days, and ER visits can last over 3 hours. At MyDoc Urgent Care, most visits are completed in less than an hour. We offer a cost-effective alternative to the ER for issues like minor injuries, infections, and illnesses. For life-threatening emergencies, such as chest pain, severe bleeding, or difficulty breathing, always call 911 or go to the nearest ER.
What about insurance?
We accept most major insurance plans for medical services, including Medicaid and Medicare. If you do not have insurance, we offer affordable self-pay rates and transparent pricing. Our staff can help you understand your benefits, answer questions about coverage, and provide cost estimates before treatment. We believe everyone should have access to quality healthcare, regardless of insurance status.
What conditions do you treat at urgent care?
We treat a wide range of conditions, including cold and flu symptoms, sore throat, ear infections, minor cuts and burns, sprains and strains, rashes, urinary tract infections, allergies, minor fractures, and more. We also provide physical exams for school, work, and sports, as well as vaccinations and on-site lab testing. If you are unsure whether we can help, call us or walk in—our team will assess your needs and provide the appropriate care or referral.
Can I get prescriptions or refills at urgent care?
Yes, our providers can prescribe medications for acute illnesses and minor conditions, such as antibiotics for infections or medications for pain relief. We can also provide short-term refills for certain maintenance medications if appropriate. Please bring a list of your current medications and any relevant medical history to your visit. For long-term medication management, we recommend following up with your primary care provider.
Do you offer pediatric urgent care?
Absolutely! Our clinics are equipped to care for children of all ages, from infants to teenagers. We understand that children have unique medical needs and strive to provide a comfortable, family-friendly environment. Our providers are experienced in pediatric care and can treat common childhood illnesses, injuries, and provide physicals and vaccinations.
What should I bring to my urgent care visit?
Please bring a photo ID, your insurance card (if applicable), a list of current medications, and any relevant medical records. If you are bringing a child, please bring their immunization records if available. Having this information helps us provide the best and safest care possible. If you have paperwork for work, school, or sports, bring that as well so we can complete it during your visit.
How do I know if I should go to urgent care or the ER?
Urgent care is appropriate for non-life-threatening conditions that need prompt attention, such as minor injuries, infections, or illnesses. If you are experiencing severe chest pain, difficulty breathing, signs of stroke, severe bleeding, loss of consciousness, or any other life-threatening emergency, call 911 or go to the nearest emergency room immediately. When in doubt, it's always better to err on the side of caution and seek emergency care.
Do I need an appointment to visit MyDoc Urgent Care?
No appointment is necessary at MyDoc Urgent Care. We welcome walk-ins at all of our locations during business hours. If you prefer, you can check in online to save time and reduce your wait. Our goal is to make healthcare as accessible and convenient as possible for you and your family.
What forms of payment do you accept?
We accept most major credit cards, debit cards, cash, and many insurance plans. If you have questions about payment or billing, our front desk staff will be happy to assist you and provide clear information about costs before your visit. We strive to make the billing process transparent and stress-free.
Can I get lab tests or X-rays at urgent care?
Yes, MyDoc Urgent Care offers on-site lab testing and X-ray services for your convenience. This allows us to quickly diagnose and treat a wide range of conditions without the need to send you to another facility. Common tests include strep throat, flu, COVID-19, urinalysis, blood work, and more. X-rays are available for injuries such as sprains, fractures, and chest concerns.
How long will my visit take?
Most visits to MyDoc Urgent Care are completed in less than an hour, including registration, evaluation, and treatment. Wait times may vary depending on the time of day and the number of patients, but we strive to provide prompt, efficient care. You can check in online to further reduce your wait time.
Can urgent care help with work or school forms?
Absolutely! We can provide physical exams for work, school, sports, and camp, as well as complete any necessary forms. Please bring any required paperwork with you to your visit. Our providers will ensure all forms are filled out accurately and promptly so you can meet your deadlines.